Without a Healthy Immune System, Too Much ‘Good’ Bacteria Can Become a Bad Thing
Research By: Theresa Alenghat, VMD, PhD | Sing Sing Way, MD, PhD | David Haslam, MD | Emily Eshleman, PhD
Post Date: February 15, 2023 | Publish Date: Feb. 15, 2023
Experts at Cincinnati Children’s find that early roots of inflammatory bowel disease may trace back to an out-of-balance relationship between gut microbiota and the developing immune system
Many people have become comfortable with the general concept of “good” (commensal) microbiota being important for digestive health. But the ways people interact with the microbes living in our gut are not so simple. New research from Cincinnati Children’s indicates that disruptions in the immune system during early life development can allow good bacteria to cause harmful outcomes.
That’s the key message of a study published in the Feb. 15, 2023, issue of the Journal of Clinical Investigation, by a team led by Theresa Alenghat, VMD, PhD, a microbiota expert in the Division of Immunobiology at Cincinnati Children’s.
The findings suggest that an infant’s developing immune system must rapidly establish a checks-and-balances system so that intestinal tissue can distinguish commensal bacteria from more dangerous invaders and react accordingly. When this process goes wrong, previously “good” bacteria can activate specific immune cells that cause tissue damaging conditions such as those observed in inflammatory bowel disease (IBD).
“We have an enormous amount of bacteria living in our intestine. They start colonizing from the moment of birth, and for most people, our immune systems do not seem to mind,” says Alenghat, who has studied the relationship between the immune system and the microbiome for years. “It has been a longstanding question in the field. How did this co-existence come about?”
This work identifies a pathway that enables that co-existence.
What is IBD?
Scientists have long believed that IBD is related to malfunctions in the immune system. These findings shed new light on how and when the developing immune system goes off-course, which in turn may eventually lead to significantly improved treatments.
About 3 million people in the United States are living with IBD, according to the federal Centers for Disease Control and Prevention. Nearly all those people have either Crohn’s disease or ulcerative colitis. The diseases can affect different parts of the intestine and colon, but they both result from inflammatory tissue damage that occurs when the body’s immune system over-reacts to otherwise normal microbes found in the gut.
Currently, treatments include surgically removing damaged parts of the intestine, and prescribing anti-inflammatory steroids, immune-suppressing drugs, biologics and other therapies. However, success has been mixed. Many patients still struggle to achieve lasting remission.
Decoding a delicate balancing act
The new study helps explain an important moment in the surprisingly deep and complex relationship between the human immune system and our gut microbiome. Eventually, this discovery could translate into ways to manipulate gut microbes to either treat IBD or prevent the condition from developing.
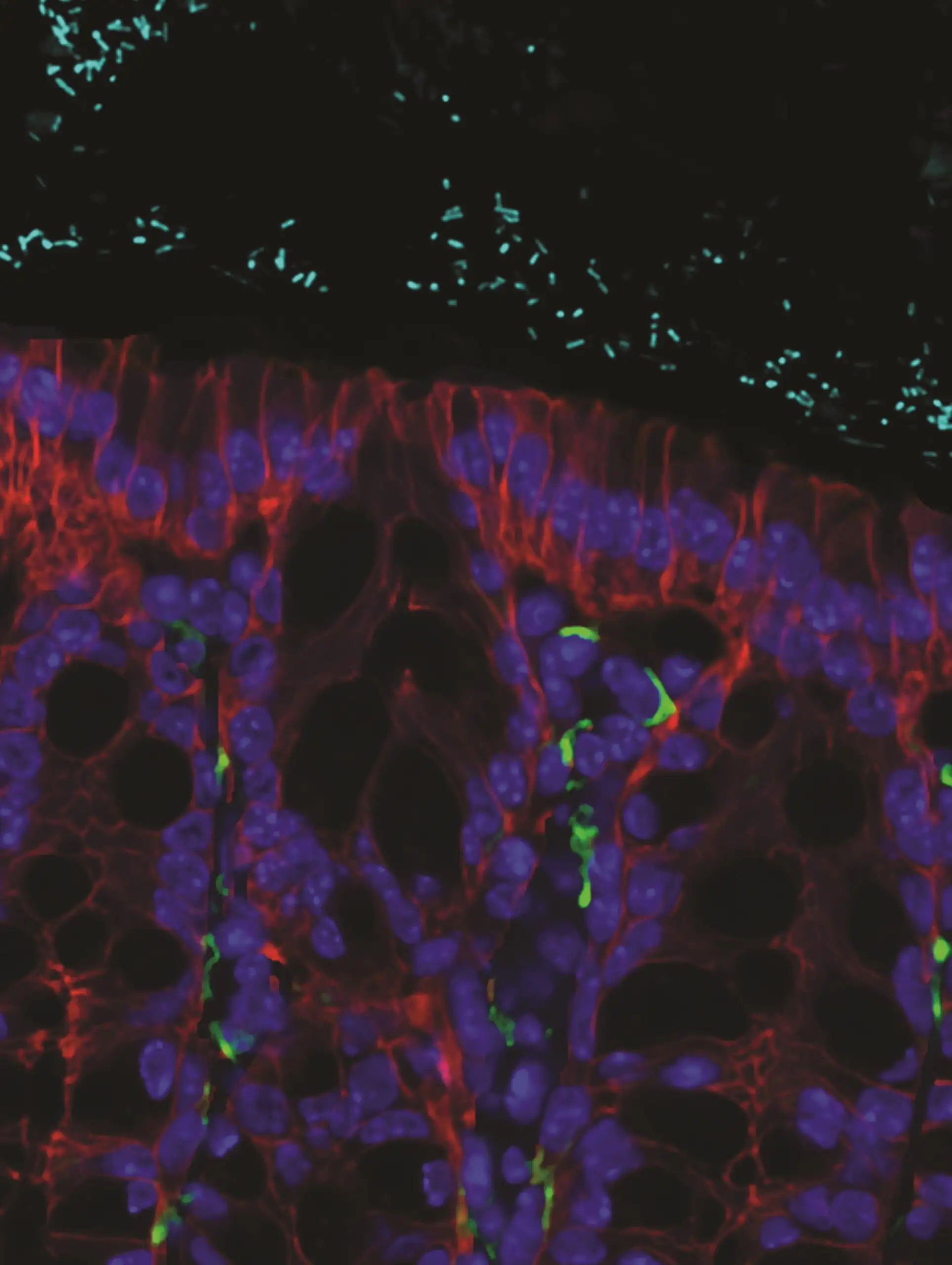
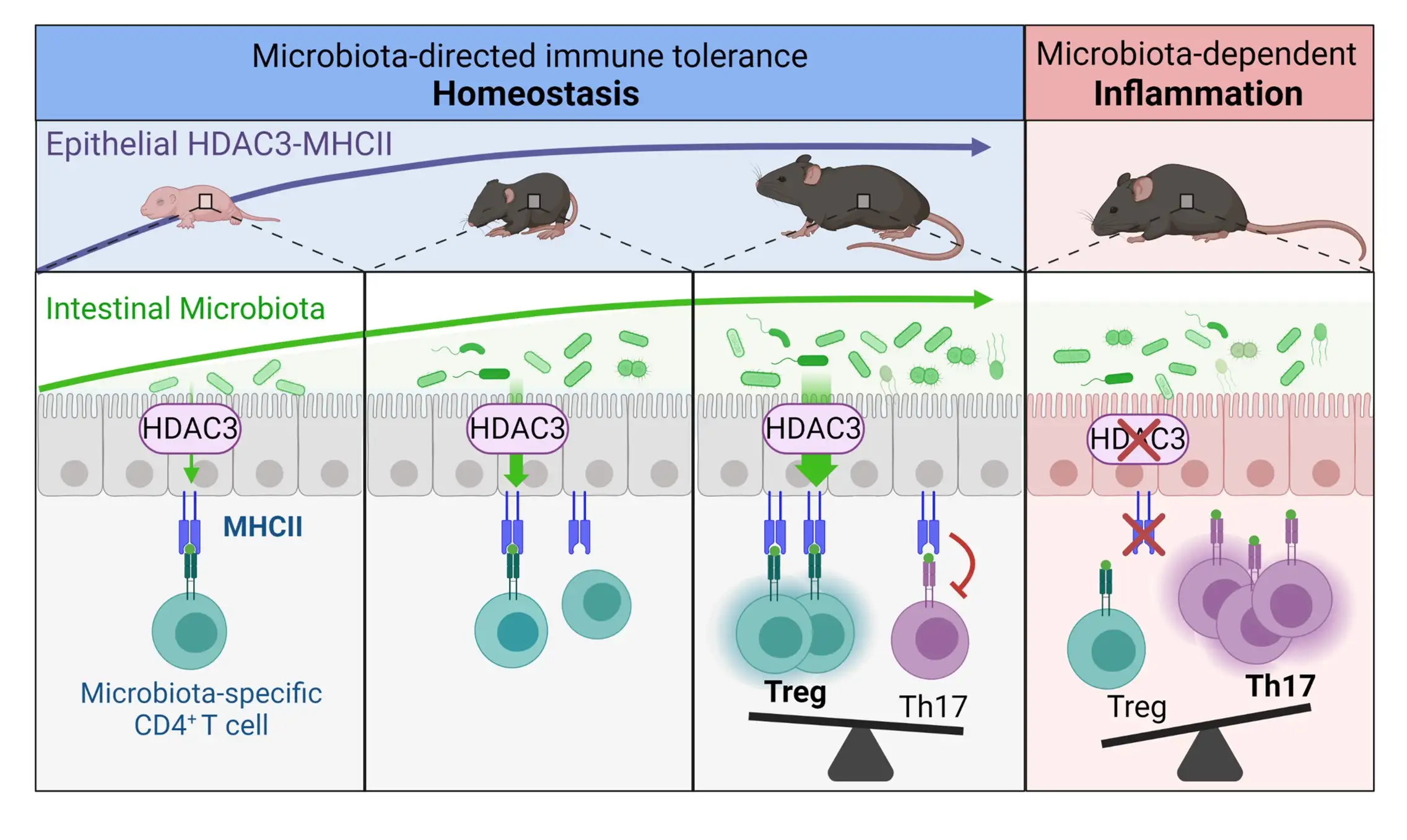
Specifically, the team reports that two proteins (HDAC3 and MHCII) located in the epithelial cells that line the intestine are key to the early formation of immune cells that recognize our microbiome.
“Elsewhere in the body, MHCII often helps activate immune cells to attack invading pathogens. But inside the lining of the intestine, MHCII limits the supply of these immune cells that can recognize and attack “good” bacteria,” says first author Emily Eshleman, PhD, research fellow in the Division of Immunobiology.
All of this immune system balancing occurs within several days after mice are born, which equates roughly to the first year of human infancy. But surprisingly, the signals that drive this process in the intestine are largely controlled by the gut microbiota.
“It’s as if the microbiome is controlling the immune responses to itself,” Alenghat says. “The microbes turn on pathways in the gut that lead to their own self-preservation.”
According to the study, this signaling pathway seems to be necessary to limit the number of immune cells that can cause inflammation in response to the microbiome.
The team verified the signaling pathway in part by comparing typical mice to those that lack the HDAC3 and MHCII genes in their gut lining epithelial cells. These mice accumulated specific cells, called T cells, in their intestine that were primed to attack commensal bacteria, which led to inflammatory tissue damage.
What does this discovery mean for people with IBD?
“Having a new understanding of a fundamental mechanism driving a disease is the first step toward finding therapeutic ways to control it,” says co-author Sing Sing Way, MD, PhD, Division of Infectious Diseases.
But much more study is needed to translate this advance into specific therapies.
Initially, this study reinforces the need to minimize disruptions during the early months of immune system formation, Way says. It also may increase interest in studying fecal microbiota transplantation (FMT) and targeting specific types of immune cells as a treatment for IBD. Both Way and Alenghat are part of the Cincinnati Children’s Center for Inflammation and Tolerance, which brings together scientists with expertise in microbiota, immune development, and inflammation.
Studies conducted in several different countries have suggested some success with FMT and Crohn’s disease remission, but in the US the effectiveness and safety of FMT for treating IBD remains under active investigation.
Longer term, “the findings support the idea that achieving personalized medicine will require taking the gut microbiome into account,” says co-author David Haslam, MD, director of the Microbial Genomics and Metagenomics Laboratory at Cincinnati Children’s.
In addition to using genetic profiles to help clinicians select the most effective treatments, people with chronic diseases may also need microbiome profiles to anticipate how well a medication might work.
About this study
Other co-authors from Cincinnati Children’s involved in the study include Tzu-Yu Shao, PhD, Vivienne Woo, PhD, Taylor Rice, Laura Engleman, Bailey Didriksen, and Jordan Whitt.
Funding sources for this study included the National Institutes of Health (DK114123, DK116868, DP1AI131080, and F32AI147591), the Public Health Service (P30 DK078392), the Kenneth Rainin Foundation, and the Burroughs Wellcome Fund.
Learn More
Watch Dr. Alenghat’s Tedx talk.
Research Fellow positions now available: Apply today
| Original title: | Intestinal epithelial HDAC3 and MHC class II coordinate microbiota-specific immunity |
| Published in: | Journal of Clinical Investigation |
| Publish date: | Feb. 15, 2023 |
Research By

The Alenghat Lab investigates epithelial and immune cell homeostasis in the context of intestinal health and disease.

My research interests include infectious diseases, reproductive biology, developmental biology and immunology.
The main focus of my research is to understand how the microbiome influences disease and contributes to health in children.

Latest Posts


About this blog
The Research Horizons blog features news and insights about the latest discoveries and innovations developed by the scientists of Cincinnati Children's. This blog does not provide medical advice, diagnosis, or treatment. Email researchnews@cchmc.org with questions or ideas.
Subscribe to Our Newsletter