Weeding Out the Toxicity of Marijuana Edibles in Pediatrics
Research By: Sheila Goertemoeller, PharmD, DABAT
Post Date: May 14, 2021 | Publish Date:
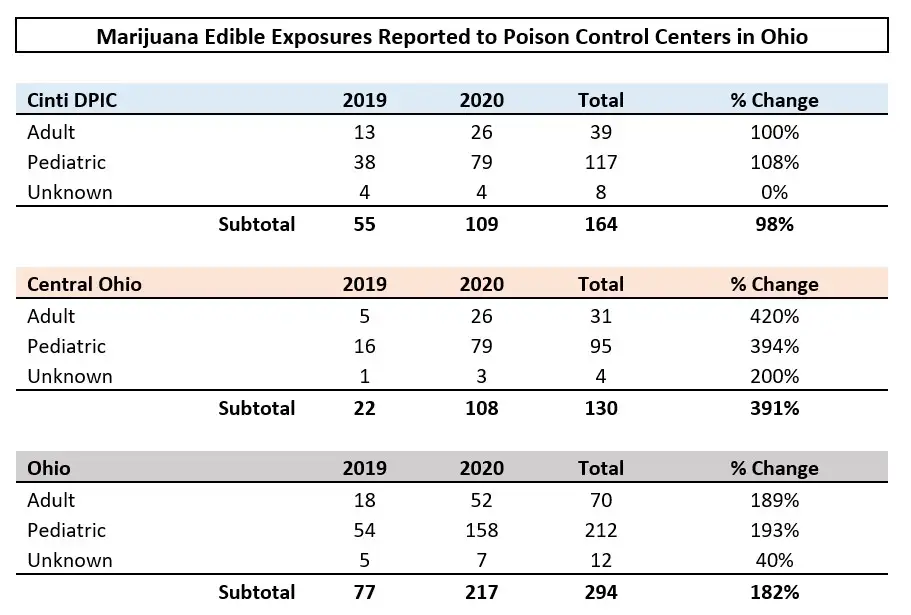
In Ohio, poison control center consults related to marijuana edibles soared 182% from 2019 to 2020.
The use of cannabis is legal in many U.S. states, whether recreational, medicinal or both. With legalization, it has become readily available in many homes. In particular, the availability of marijuana edibles in enticing forms has led to exposures in vulnerable pediatric patients. These exposures have resulted in an increase in calls to poison control centers, emergency department (ED) visits and hospitalizations.
The Drug and Poison Information Center (DPIC) at Cincinnati Children’s is one of two such centers in Ohio, each covering approximately half of the state’s population.
The centers provide toxicology consults for exposures to all cannabis products, including edibles. In the last few years, poison control center calls on edibles have steadily increased.
- In the state of Ohio, poison control center consults were provided on 217 cases in 2020, a 182% increase from 77 cases in 2019.
- From the Cincinnati center, 109 consults were provided in 2020, which was a 98% increase from 55 consults in 2019. Of our 109 consults in 2020, 72% involved adolescents and children.
- Among the 208 pediatric exposures that could be followed in 2019 and 2020, 84% (n=176) were cared for in an emergency department setting. Of these, approximately 25% were admitted for observation and care, including 10% who required intensive care.
- No deaths among children consuming excessive amounts of marijuana edibles were reported in 2019 or 2020.
Read news coverage at Cincinnati.com (subscribers only)
These consults were requested from health care professionals and the public. Most calls from health care professionals were to obtain information about toxicity and patient management, whereas calls from the public were to determine if a patient needed to seek medical care.
Overdoses from edibles on the rise
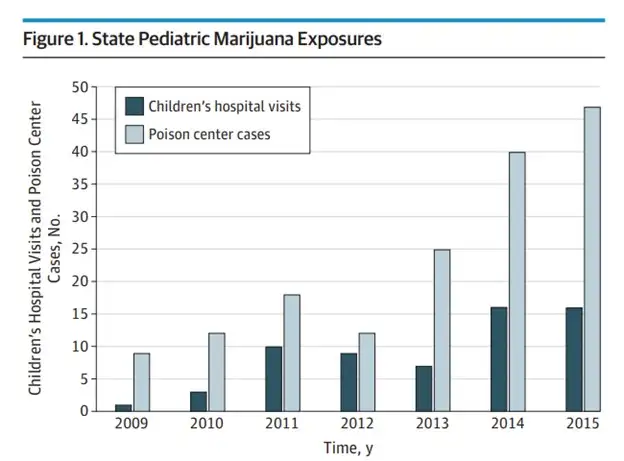
In a study done by the Children’s Hospital of Colorado and the Rocky Mountain Poison & Drug Safety Center from 2009-2015, published in JAMA Pediatrics, about 50% of cannabis exposures in children at or under 9 years old were edible products.
Another study, published in Clinical Toxicology, was done by the Oregon/Alaska poison center with data from December 2015-April 2017 (recreational use was legalized in 2014 in Oregon and 2015 in Alaska). It showed that in children under 12 years old, 97% of cannabis exposures were due to ingestion, and two-thirds of these were edible products. Meanwhile in Massachusetts, post medical marijuana legalization, it was noted that in kids under 5-years-old, most exposures were to edibles and extracts rather than the plant material.

Covid and edibles
There are news reports that, since the pandemic began in March 2020, the cannabis industry has seen an influx of customers, many seeking to buy the cannabis in edible form Weed Edibles Are Selling Well During the Pandemic – The New York Times (nytimes.com)
Prevention and awareness
The Substance Abuse and Mental Health Services Administration (SAMHSA) observes National Prevention Week on May 9-15. This week is a public education platform to promote prevention through providing resources and ideas to help communities and individuals.
From a public health view, prevention can play an important role in keeping children safe from accidental edible exposures. Educating families on storing products away from children’s reach and sight can be a simple but important measure. Some states have taken steps to prohibit certain edible products and institute THC dose limits, warning symbols, detailed labeling and child resistant packaging.
FOR FAMILIES: 4 Must-Know Facts About Marijuana Edibles
For health professionals, understanding more about the wide variety of chemical compounds and concentrations that can be found in marijuana edibles may help provide the most timely and appropriate care for patients facing potential overdoses.
One plant, many chemicals
Cannabis plants contain many chemical compounds including flavonoids, terpenes, and cannabinoids. The cannabinoids are a class of compounds that act upon the endocannabinoid system.
The two main G protein-coupled receptors that act on this system are the CB1 (central nervous system) and CB2 (immune cells, neurons, gastrointestinal tract) receptors. We have yet to elucidate the activity of all the cannabinoids, but two in particular are well studied: tetrahydrocannabinol (THC) and cannabidiol (CBD).
THC vs. CBD
∆-9 THC is the principle psychoactive constituent of cannabis. In its synthetic form it is the active ingredient in dronabinol (Marinol®), which is approved for anorexia in AIDS patients and for chemotherapy-induced nausea and vomiting. THC is a partial agonist at CB1 (responsible for psychoactive effects) and CB2 receptors.
CBD is devoid of psychoactive properties. Cannabidiol (Epidiolex®) has been approved for Lennox-Gastaut syndrome, Tuberous sclerosis syndrome and severe myoclonic epilepsy in infancy. CBD does not bind CB1 and appears to negatively modulate it.
THC formulations and potency
The formulation and route of cannabis has an impact on potency. The most common route of exposure has traditionally been smoking the classic herbal plant material.
Today, several formulations with varying THC content exist, including extracts (waxes, hashish, tinctures, and refined oils), edibles (candies, baked goods, beverages, lozenges, pills) and topicals (cream, lotions, spray, patches).
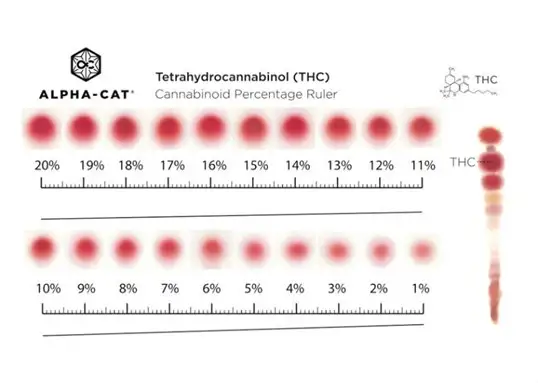
The THC content in cannabis products from the mid-90s was ~4%. Currently, plant material grown in Ohio may contain up to 35 % THC, and processed edibles may contain as much as 70% THC. Products aimed for medical use often have THC content exceeding that for recreational use.
THC content measurement methods vary within the industry, making it nearly impossible for a user to determine how much to use across the various products and formulations. Marijuana test kits are commercially available and marketed for users to measure the potency of their purchased cannabis products.
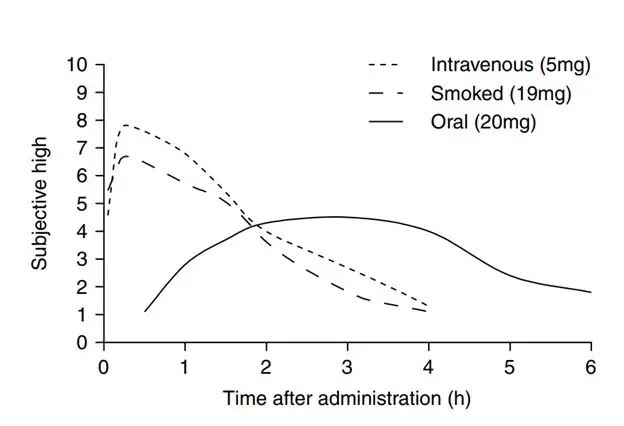
THC kinetics
The pharmacokinetics of THC varies based on the route. When smoked, THC has an onset of 10 minutes, with a peak of 20-30 minutes, and overall duration of 45-60 minutes. When ingested, the onset is delayed to about 60 minutes; peaks occur between 120-240 min., and in some cases as long as 300 minutes; and overall duration can be 24 hours.
While pharmacokinetics are somewhat established, toxicokinetics are poorly understood. With the slower onset of the ingestion route, a larger dose may be consumed before experiencing adverse effects.
Toxic dose of THC in edibles
An edible is THC extract infused in food or drinks which can resemble otherwise harmless candies, cookies or beverages.
Determining the dose ingested is often difficult in edible ingestions due to varying THC content, serving size and individual patient characteristics. For adult users a recommended “starting dose” is about 10mg. A non-toxic or minimally toxic dose in a child is not clearly defined.
In one study, a dose-response analysis was conducted comparing severity of intoxication in THC-naïve children (n=38) compared to THC non-naïve children (n=38). Inclusion criteria was 31 months to 20 years of age, treated for an acute unintentional marijuana ingestion, without concomitant substances. The dose-response analysis consisted of eight patients in the naïve group.
Children with estimated doses at or less than 3 mg/kg were likely to be observed in the emergency room but not admitted. Children with doses of above 5 mg/kg were likely to be admitted.
The dose associated with floor admission was 7 mg/kg (± 4). The doses resulting in intensive care admission was 13 mg/kg (± 9).
It was noted that in the naïve group, patients had a higher incidence of lethargy and longer duration of hospitalization. The non-naïve patients had a higher incidence of cognition issues.
Toxicity and management of edible ingestions in pediatrics
The semblance between edibles and candy can increase the likelihood of rapid overdose often in large amounts. A candy bar can often be several servings for an adult user.

The most common toxicity seen in pediatric patients from edibles is lethargy. Other reported effects include ataxia, mydriasis, tachycardia, red eyes, nausea, vomiting, confusion, agitation and respiratory depression, as well as case reports of seizures.
Data from the Children’s Hospital of Colorado indicated that 35% of children presenting to the ED were admitted, 41% of them requiring a pediatric ICU.
The mainstay of treatment is symptomatic and supportive care until patients return to baseline. It is important to do a thorough evaluation for other causes of CNS depression, and comorbidities should be assessed.
Cannabis exposures should be part of the differential in an altered child who presents with sedation and ataxia of unknown cause. Social work evaluation may need to be considered depending on the exposure scenario.
Resources available
Health care professionals play a key role in the management of pediatric marijuana edibles. The Drug and Poison Information Center at Cincinnati Children’s is staffed 24/7 with board-certified medical toxicologists, clinical toxicologists, and pharmacists/nurses who are specialists in poison information.
Call DPIC: 1-800-222-1222
For information on how parents can help keep edibles away from children, visit healthychildren.org.
Read more about potential drug-drug interactions for children with tuberous sclerosis complex
Read more about potential links between marijuana use during pregnancy and preeclampsia
References
Kathy T. Vo, Howard Horng, Kai Li, Raymond Y. Ho, Alan H. B. Wu, Kara L. Lynch, Craig G. Smollin. Cannabis intoxication case series. Annals of Emergency Medicine 2018; 71(3) 306-313 Cite Unintentional cannabis ingestion in children a systematic review
Grotenhermen, Franjo. Pharmacokinetics and pharmacodynamics of cannabinoids. Clin Pharmacokinet 2003 42: 327-360
Heizer JW, Borgelt LM, Bashqoy F, Wang GS, Reiter PD. Marijuana Misadventures in Children: Exploration of a Dose-Response Relationship and Summary of Clinical Effects and Outcomes. Pediatr Emerg Care. 2016 Apr 5.
George Sam Wang, MD; Marie-Claire Le Lait, MS; Sara J. Deakyne, MPH; Alvin C. Bronstein, MD; Lalit Bajaj, MD, MPH; Genie Roosevelt, MD, MPH. Unintentional pediatric exposures to marijuana in Colorado, 2009-2015. JAMA Pediatr. 2016; 170 (9)
Research By



Latest Posts

{kind=link}
About this blog
The Research Horizons blog features news and insights about the latest discoveries and innovations developed by the scientists of Cincinnati Children's. This blog does not provide medical advice, diagnosis, or treatment. Email researchnews@cchmc.org with questions or ideas.
Subscribe to Our Newsletter